On December 31st 2019, China reported to the World Health Organisation (WHO) 44 cases of acute pneumonia that were of an unknown cause; out of these cases, 11 patients were severely ill. As of today, 5th January 2020, this number has risen to 59 with cases being seen in other regions such as Hong Kong. To understand why this is suspicious and alarming, we have to take ourselves back to the SARS (severe acute respiratory syndrome) outbreak of 2003.
The SARS coronavirus outbreak infected 8,098 people worldwide, with 774 of those dying after contracting it. Thankfully, after counter measures were put in place to prevent transmission and contagion, including the use of more than 800 medical experts and chemical testing to identify the cause of the disease, the virus pretty much went down without a proper fight.
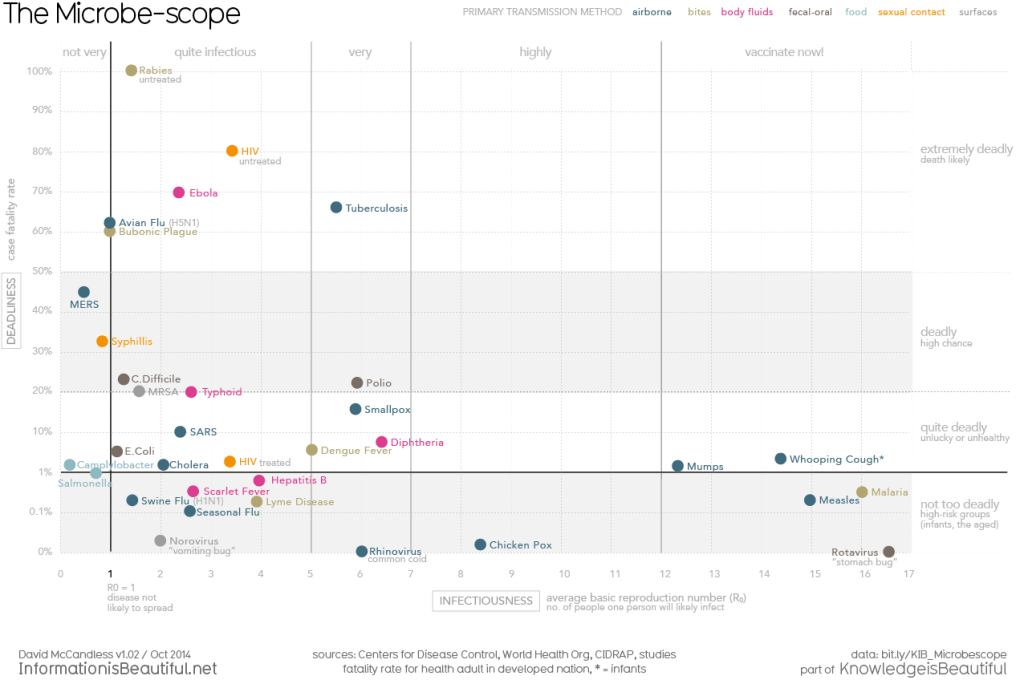
When we talk about a viruses pathogenic ability, we refer to two aspects: how transmissible it is from host to host and how deadly it is (mortality rates). The SARS virus didn’t become more than an epidemic because it wasn’t particularly efficient at transmitting between hosts and also killing them. In fact the only reason it managed to spread from China to other countries such as America and Hong Kong, is due to the lack of transparency of the Chinese Government.
In fact, when the outbreak occurred the PRC (Peoples Republic of China) forced a lower coverage of the events by the press and also waited until over 10 people died until they fully reported it to the WHO. As a result, the Chinese health minister, Zhang Wenkang, was sacked and the WHO brought together 196 countries to better improve their ‘capacity to detect, assess, notify and report public health events including outbreaks’. As of 2014, only 1/3 of these countries have achieved this target.
2003’s SARS epidemic showed us that on an international level, we are not ready to logistically communicate with one another in order to deal with another outbreak. The concern with the current ‘atypical pneumonia’ outbreak is that there is a possibility that history is repeating itself and countless lives could be loss due to the same mistakes that have been made in the past. Hopefully this turns out not to be the case.
Sources: https://www.cdc.gov/sars/about/fs-sars.html#outbreak, https://www.who.int/ , https://www.japantimes.co.jp/news/2019/12/31/asia-pacific/science-health-asia-pacific/outbreak-sars-like-pneumonia-investigated-china/ , https://en.wikipedia.org/wiki/Timeline_of_the_SARS_outbreak